How to write DAP notes (with a therapist-ready example)
Most clinicians don’t lose time to the actual writing. They lose it to the deciding — what to keep, where it goes, how much detail is enough. DAP notes are popular precisely because they reduce that friction: three sections, a clear logic, and no wasted compartments. If you’ve ever stared at a SOAP template wondering whether something belongs in “Subjective” or “Objective,” DAP offers a cleaner path. This guide walks through what each section is for, how DAP differs from SOAP, and a short worked example you can adapt to your own caseload.
What DAP stands for
DAP is a progress-note format built around three parts:
- Data — what happened in the session: what the client reported, what you observed, what interventions you used.
- Assessment — your clinical thinking: how you interpret the data, progress toward goals, risk, working hypotheses.
- Plan — what comes next: the next appointment, homework, referrals, changes to the treatment plan.
The format is common in counseling, social work, and behavioral health settings. Its appeal is the merged first section: instead of separating what the client said from what you saw, DAP keeps the whole observable picture together and reserves a distinct space for your interpretation.
Data: the observable record
The Data section is everything that could, in principle, be witnessed or reported. It’s descriptive, not interpretive. Think of it as the part of the note another clinician could read and broadly agree with, because it sticks to what occurred.
Include things like:
- Client report — presenting concerns, mood, events since the last session, in the client’s own framing.
- Observable presentation — affect, appearance, engagement, notable behavior (“arrived on time, tearful when describing work conflict”).
- Interventions delivered — what you actually did: cognitive restructuring, a grounding exercise, psychoeducation about the stress response.
- Relevant content — themes, disclosures, or topics that carry clinical weight.
The discipline here is to resist interpreting too early. “Client seemed anxious” is a small judgment; “client spoke rapidly, shifted in the chair, and described difficulty sleeping” is data. Save the inference for the next section. Whether you capture this by dictation or by recording the session shapes how raw your Data will be — if you’re weighing those approaches, our note on dictation versus recording therapy sessions lays out the tradeoffs.
Assessment: your clinical reasoning
This is where you, the clinician, do the thinking the Data can’t do on its own. The Assessment connects what happened to why it matters: progress toward treatment goals, your working understanding of the client’s presentation, any shifts in functioning, and risk.
A strong Assessment usually touches:
- Progress — movement toward (or away from) stated goals since the last session.
- Clinical interpretation — how the session’s content fits your conceptualization.
- Risk and safety — present or absent; if relevant, what you assessed and concluded.
- Diagnostic relevance — symptoms that support, refine, or complicate the working diagnosis.
The Assessment is the section that most clearly reflects your expertise, and it’s the one a reviewer, auditor, or future treating clinician will read most carefully. Keep it defensible: tie each judgment back to something in the Data.
Plan: what happens next
The Plan is concrete and forward-looking. It answers: what did we agree to, and what are you doing about it? At minimum, note the next session or interval, any between-session work, and changes to the treatment direction.
Useful elements:
- Next contact — frequency or scheduled date.
- Homework or practice — anything assigned, in enough detail to follow up.
- Treatment adjustments — new goals, a shift in modality, a referral or consult.
- Coordination — releases, collateral contacts, or follow-up with a prescriber.
DAP notes versus SOAP, briefly
SOAP splits the first half of the note into Subjective (what the client reports) and Objective (what you observe and measure). DAP folds both into Data. For talk therapy, where “objective” vitals and labs are rare, that merge often feels more natural and avoids the recurring question of which bucket a given detail belongs in.
| SOAP | DAP | |
|---|---|---|
| Sections | Subjective, Objective, Assessment, Plan | Data, Assessment, Plan |
| First section | Splits report from observation | Combines both as Data |
| Common fit | Medical, integrated care | Counseling, behavioral health |
Neither is more “correct.” If you want to see the four-part structure side by side with full write-ups, our SOAP note examples cover that format in depth. Your payer, agency, or licensing board may prefer one, so it’s worth confirming, since documentation requirements vary by jurisdiction and setting and this isn’t legal advice.
A short worked example
A pseudonymous client, “R.,” in week six of treatment for generalized anxiety:
Data: R. arrived on time, reported a “rough week” after a conflict with a manager. Described racing thoughts and three nights of disrupted sleep. Tearful when recounting the meeting. Engaged throughout; practiced a paced-breathing exercise in session and identified two catastrophic thoughts.
Assessment: Anxiety symptoms elevated relative to last session, tied to an identifiable workplace stressor rather than a generalized escalation. R. is increasingly able to name cognitive distortions in the moment — progress toward the cognitive-flexibility goal. No safety concerns; denied SI when asked.
Plan: Continue weekly. Homework: thought record for two workplace situations. Revisit sleep hygiene next session. No change to working diagnosis.
Notice how each Assessment claim points back to something in the Data — that traceability is what makes the note hold up.
Where drafting tools fit
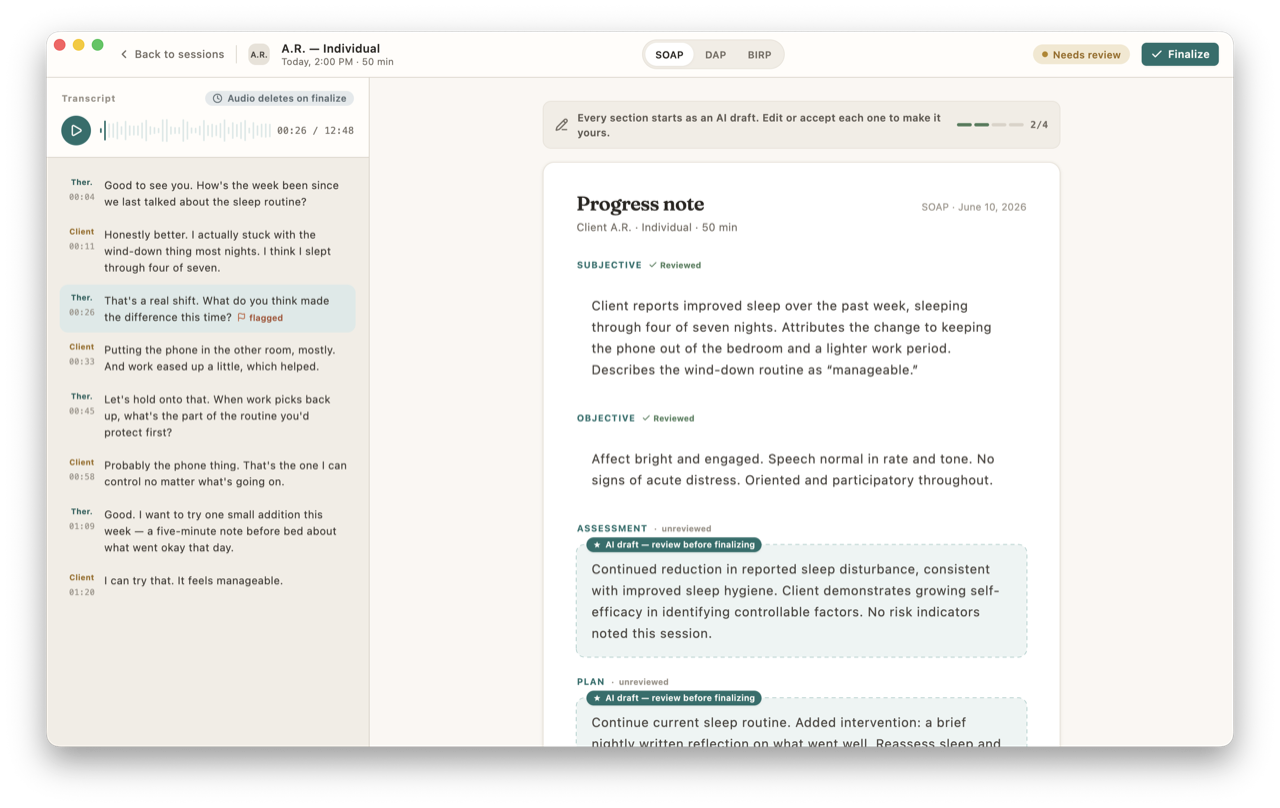
A note that follows this structure reliably is a candidate for assistance. CouchNotes transcribes the session on your Mac and generates a DAP draft that already separates Data, Assessment, and Plan — but it’s a starting point, not a finished note. You read it, correct what’s wrong, sharpen the Assessment in your own clinical voice, and sign it. The draft saves typing; the judgment, and the authorship, stay yours. The processing happens on-device, so the session content never leaves your machine — there’s no cloud, no account, and no telemetry.
DAP rewards clarity over volume. A note that keeps observation, reasoning, and next steps in distinct lanes is faster to write, easier to defend, and more useful to the next clinician who reads it — including future you, three months from now, trying to remember what “R.” was working through.